
New SMN-boosting Molecule Shows Promise as Add-on Therapy
Written by |

Targeting a specific region of an intermediate molecule generated from the SMN2 gene increased the levels of functional SMN — the protein lacking in spinal muscular atrophy (SMA) — in cells derived from SMA patients, a study shows.
In addition, combining this approach with a splicing modifier similar to Spinraza (nusinersen) resulted in even greater SMN levels than treatment with the splicing modifier alone.
These findings highlighted the therapeutic potential of targeting this region, called 5′ untranslated region, especially when combined with currently-approved splicing modifier therapies.
Future studies are needed to better understand the underlying mechanisms of this new approach and to test it in a mouse model of SMA before being able to move to clinical trials, the researchers noted.
The study, “Targeting the 5′ untranslated region of SMN2 as a therapeutic strategy for spinal muscular atrophy,” was published in the journal Molecular Therapy – Nucleic Acids.
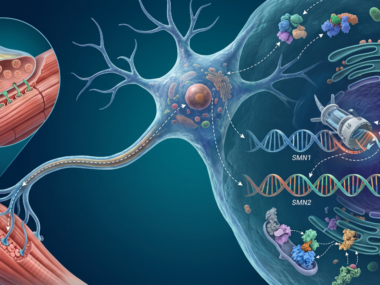
SMA is caused by low to no levels of SMN, a protein essential for motor neuron and muscle health, due to mutations in the SMN1 gene. While a “backup” gene, SMN2, is capable of producing SMN, a slight difference in its DNA sequence results in an event called “alternative splicing” that limits the amount of functional SMN it produces to 10%–15%.
Alternative splicing allows for a single gene to give rise to many different proteins. Just like in a recipe, adding or removing certain key ingredients — in this case, sections of genetic information called exons — can change the results: the messenger RNA (mRNA) and the final protein. (mRNA is a molecule derived from DNA and used as a template for protein production.)
In SMN2, this event causes the loss of exon 7 from most of its mRNA molecules, resulting in a shorter, poorly functioning SMN protein.
Both Spinraza and Evrysdi (risdiplam), two of the three therapies currently approved for SMA patients, work by preventing exon 7 deletion from SMN2 mRNA, correcting its splicing and increasing the production of a functional SMN protein.
However, “targeting splicing as a means of increasing SMN levels has a ceiling effect determined by the abundance of SMN2 transcripts [mRNA molecules] in cells,” the researchers wrote.
As such, increasing the total pool of SMN2 mRNA and boosting the mRNA-to-protein process are two potential strategies to amplify the effects of splicing modifiers.
Researchers at the National Institute of Neurological Disorders and Stroke, and the University of Oxford have now discovered that targeting a specific region of SMN2 mRNA, called 5’ untranslated region, may be a potential add-on therapy for splicing modifiers.
This region, present at the beginning of mRNA molecules of every gene, is known to contain regulatory elements that influence protein production by controlling mRNA’s stability and localization, as well as the efficiency of the mRNA-to-protein process.
The team designed six antisense oligonucleotides (ASOs) targeting different sequences in the 5’ untranslated region of SMN2 mRNA. ASOs, like the one comprising Spinraza, are man-made single-stranded RNA molecules designed to be complementary to the target mRNA, changing the final molecule and the resulting protein.
When treating SMA patient-derived cells grown in the lab with each of these ASOs, the team found that ASO#1, the one targeting the most upstream mRNA sequence, resulted in the greatest increase in SMN levels (up to 3.7 times).
Further tests revealed that ASO#1 raised SMN levels by increasing SMN2 mRNA’s stability, thereby preventing its degradation and increasing the number of mRNA molecules available for protein production.
Notably, this was accompanied by an increase in the levels of full-length mRNA, including exon 7, in patient-derived cells, but not in cells derived from SMA carriers.
Typically healthy, SMA carriers have only one mutated SMN1 gene copy and can transmit the mutated gene to their children. A child needs to inherit two defective SMN1 copies — one from the mother and one from the father — to develop the disorder.
Based on the different effects in patients and carriers, and given the fact that SMN is involved in the formation of the splicing machinery (spliceosome), the team hypothesized that in states of SMN and spliceosome deficiency, an increase in SMN levels may alter its own splicing.
“We suspect that the increased level of total SMN mRNA is a direct effect of the 5′ UTR [untranslated region] ASO, whereas increased exon 7 inclusion is more likely due to SMN feedback,” the researchers wrote.
Moreover, the team found that treating patient-derived cells with a combination of ASO#1 and a splicing modifier similar to Spinraza resulted in significantly higher SMN levels than those achieved when treating cells with the splicing modifier alone.
However, the team speculated that the combination treatment would not be superior to ASO#1 alone since it already promotes splicing correction with a shift toward full-length mRNA.
“Our results add to the current understanding of SMN regulation and point toward a new therapeutic target for SMA,” the researchers wrote.
The team is now conducting further work to clarify the new ASO’s mechanism of action, which may reveal that this type of approach can be used to restore the levels of proteins missing in other diseases, such as Duchenne muscular dystrophy.
Of note, a patent application has been filed for the 5′ UTR ASOs described in the study, and one of the researchers is a founder and shareholder of PepGen, a therapeutics company targeting severe neuromuscular diseases.

Leave a comment
Fill in the required fields to post. Your email address will not be published.